Gold Coast Elbow Surgeon Dr Michael Maguire performs arthroscopic tennis elbow surgery or Common Extensor Origin Release and Repair. He also offers arthroscopic Golfer’s Elbow Surgery or Common Flexor Origin Release and Repair.
Most cases of tennis elbow and golfer’s elbow will respond to non-operative measures including "Counter Force Bracing”, a structured therapy program and time. Infact with a structured rehabilitation program the majority of tennis elbow and golfer’s elbow cases will respond favourably.
Unfortunately, it is difficult to predict how long it will take for "Tennis Elbow" or Lateral Epicondyltis symptoms to resolve. In come cases it may take years to settle. The same is true for Golfer’s Elbow.
If you are suffering from Tennis Elbow or Golfer’s Elbow and have not responded to the usual non-operative measures then surgery may be appropriate particularly if a "Tear of the Common Extensor Origin or Common Flexor Origin" is diagnosed on Ultrasound Scan.
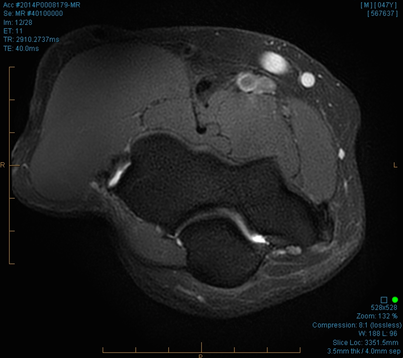
MRI is very helpful in the diagnostic work-up especially in questionable cases of Tennis Elbow and Golfer’s Elbow or to confirm the presence of a CEO (Common Extensor Origin) Tear or CFO (Common Flexor Origin) Tear. Ultrasound scans lack the sensitivity and specificity to differentiate CEO or CFO tears from tendinosis in some cases.
The 3T MRI scan below of the elbow clearly shows tearing of the CEO in both coronal and axial sequences.

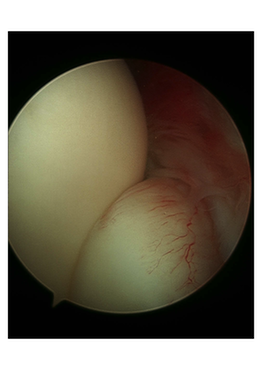
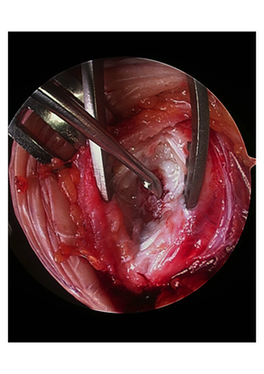
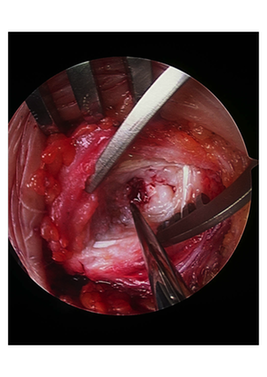
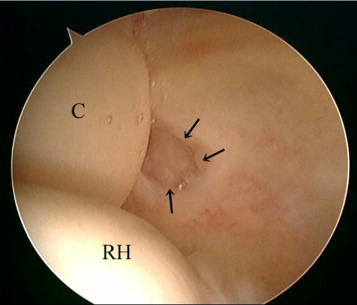
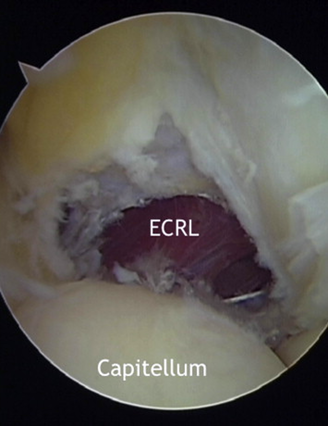
Dr Maguire performs a diagnostic elbow arthroscopy to exclude other causes of lateral or medial elbow pain. He then confirms the torn ECRB tendon (CEO Tear) or Torn CFO and localises the exact site of the pathology which often can be seen quite clearly at arthroscopy (see photo below).
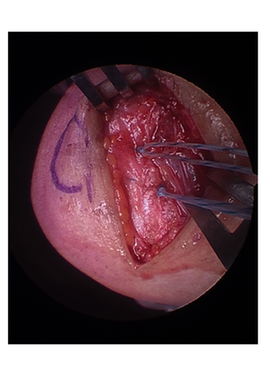
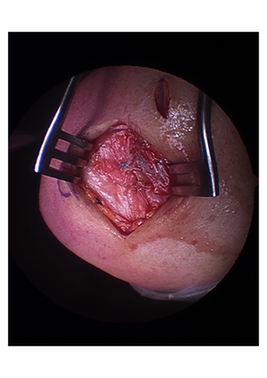
Dr Maguire will then either debride the tear arthroscopically or perform a "mini-open" release/excision and repair through a small 2cm incision. This surgery is almost always able to be done as a "Day Case".

The success rate of this type of surgery is in the order of 90% or more, particularly if the "Nirschl Lesion" or degenerate ECRB tendon tissue can be found and excised. With a "mini-open" approach the tissues can be easily repaired, suturing healthy tissue to healthy tissue.
Dr Maguire uses suture anchors to repair the torn tissue anatomically back to the bone.
Following surgery for tennis elbow patients may move their wrist and elbow immediatley and start on a gradual strengthening programme. Only a sling for comfort is required post op for 1-2 days. Most patients have recovered from their surgery in a matter of weeks and usually return to full activity by about 2-3 months post operatively.
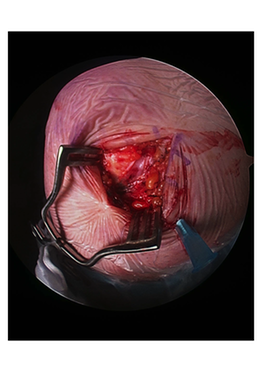
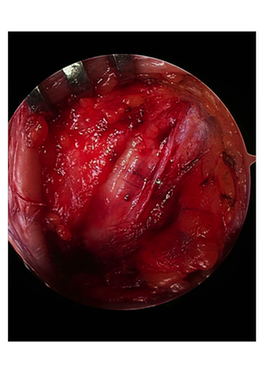
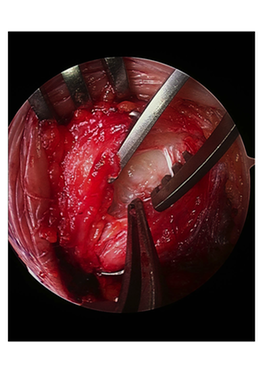
Below actual case showing localisation of tear arthroscopically and mini-open approach. CEO Tear and epicondyle debrided and microfracture performed to encourage "pluripotent cells (similar to stem cells) from marrow to enter repair site. Repair then performed with one or two suture anchors to restore "foot print" repair to bone. Solid repair allows early Range of Motion and accelerated rehab post operatively.