


What is the rotator cuff?
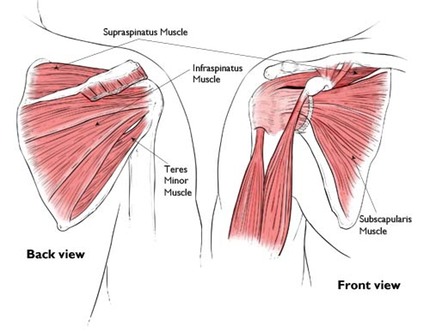
The rotator cuff is a group of four muscles and their tendons which "surround" the shoulder joint. These muscles are the supraspinatus, subscapularis, infraspinatus and teres minor.
What does the rotator cuff do?
The rotator cuff, as it's name suggests rotates the shoulder. The subscapularis at the front of the scapula (shoulder blade) rotates the arm internally, whilst the infraspinatus and the teres minor at the back rotate the arm externally.

The supraspinatus which sits on the top of the scapula above the spine of the scapula is the main muscle responsible for initiating elevation of the arm. The tendon of the supraspinatus is most commonly torn.
If a supraspinatus tendon tear is large enough some people are unable to elevate the arm. This is known as "pseudoparalysis" of the shoulder. The deltoid simply makes the shoulder shrug superiorly. This can lead to superior escape of the shoulder's humeral head.

Together the four rotator cuff muscles/tendons dynamically stabilise the shoulder as it moves, keeping the humeral head (ball) "centred" in the glenoid (socket).
What is Rotator Cuff Arthropathy?
Rotator cuff arthropathy is caused by a failure of the rotator cuff to adequately contain the humeral head in the glenoid. Usually a massive tear of the rotator cuff which has not healed after surgical repair or if not repaired at all will lead to a progressive arthritis in the shoulder.
Patients develop a characteristic shrugging type of movement when they attempt to elevate the shoulder. This caused by the deltoid muscles line of pull.
Eventually the cartilage at the superior aspect of the glenoid becomes eroded and the humeral head starts articulating with the acromion.
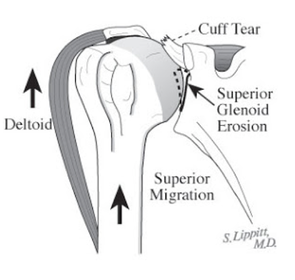
The x-ray appearance of a shoulder with cuff arthropathy is quite characteric. Note how the humeral head appears to be articulating and actually eroding or re-shaping the acromion.

When to refer early?
1) If pain severe and unrelenting despite non-op treatment such as corticosteroid injections and physio.
2) If patient has pseudoparalysis and can't elevate arm above shoulder height.
3) If the erosion and thinning of the acromion becomes severe enough that it may fracture or lose the attachment of the deltoid muscle. This scenario makes the success of a Reverse Shoulder Replacement somewhat less predictable or may not allow the surgery to be done at all.


If you see an x-ray like this with thinning of the acromion refer early to an upper limb surgeon!!